
New enVista Specification Sheet: Click Here
Glistenings do exist, but not for enVista (1).
 enVista is a new Glistening-free, hydrophobic acrylic IOL from Bausch + Lomb.
enVista is a new Glistening-free, hydrophobic acrylic IOL from Bausch + Lomb.
No glistenings were reported at any time in controlled clinical studies (1,3,4)
Aberration-free aspheric Advanced Optics (8-10)
Designed to minimize PCO (11)
Give your patients long-term clarity and quality of vision (2-10)
No glistenings were reported at any time in controlled clinical studies (1,3,4)
Aberration-free aspheric Advanced Optics (8-10)
Designed to minimize PCO (11)
Exceptional quality of vision
No glistenings were reported at any time in controlled clinical studies (1,3,4)
Glistenings are prevented and material stability enhanced by:Hydrating the lens to equilibrium water content so that it will neither gain nor lose water
Packaging the lens in 0.9% saline solution to eliminate fluid exchange with the aqueous humor (3,5-7)
Abrasion resistance is increased due to improved surface durability (7)
Hydrophobic properties are maintained over time (5)
Enhanced contrast sensitivity; uniform power, center to edge; and better vision quality are delivered by Bausch + Lomb aspheric, aberration-free Advanced Optics (8-10)
Designed to minimize PCO
Step-vaulted haptics are designed to vault the optic posteriorly for direct contact with the capsular bag
LEC migration inhibited by 360° square barrier edge (11)
Stability and advanced control
100% of patients had ≤ 5° of IOL rotation between days 30 and 180 (1)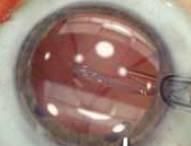
Precise positioning in the capsular bag and removal of viscoelastic are facilitated by controlled unfolding.
References
1. Bausch & Lomb Incorporated Study #658 - “A Prospective Multicenter Clinical Study to Evaluate the Safety and Effectiveness of a Bausch + Lomb One Piece Hydrophobic Acrylic Intraocular Lens in Subjects Undergoing Cataract Extraction.” Final Clinical Study Report, dated 24 Aug 2011.
2. Dhaliwal DK, Mamalis N, Olson RJ, et al. Visual significance of glistenings seen in the AcrySof intraocular lens. J Cataract Refract Surg. 1996;22(4):452-457.
3. Tetz MR, Werner L, Schwahn-Bendig S, Battle JF. A prospective clinical study to quantify glistenings in a new hydrophobic acrylic IOL. Paper presented at: American Society of Cataract and Refractive Surgery (ASCRS) Symposium & Congress; April 3-8, 2009; San Francisco, CA.
4. enVista™ Directions for Use.
5. Data on file, Bausch & Lomb Incorporated. Mentak K et al. MD-14 lens material a novel polymer for IOL applications.
6. Data on file, Bausch & Lomb Incorporated. Martin P, Elachchabi A, Goldberg E, Mentak K. Atomic force microscopy (AFM) of IOL surface morphology for
dry and hydrated hydrophobic acrylic IOLs. Study Report, July 27, 2006.
7. Mentak K, Martin P, Elachchabi A, Goldberg E. Nanoindentation studies on hydrophobic acrylic IOLs to evaluate surface mechanical properties. Paper presented at: XXV Congress of the European Society of Cataract & Refractive Surgeons (ESCRS); September 8-12, 2007; Stockholm, Sweden.
8. Santhiago MR, Netto MV, Barreto J Jr, et al. Wavefront analysis, contrast sensitivity, and depth of focus after cataract surgery with aspherical intraocular lens implantation. Am J Ophthalmol. 2010;149(3):383-389.
9. Pepose JS, Qazi MA, Edwards KH, Sanderson JP, Sarver EJ. Comparison of contrast sensitivity, depth of field and ocular wavefront aberrations in eyes with an IOL with zero versus positive spherical aberration. Graefe’s Arch Clin Exp Ophthalmol. 2009;247(7):965-973.
10. Johansson B, Sundelin S, Wikberg-Matsson A, Unsbro P, Behndig A. Visual and optical performance of the Akreos® Adapt Advanced Optics and Tecnis Z9000 intraocular lenses: Swedish multicenter study. J Cataract Refract Surg. 2007;33(9);1565-1572.
11. Nishi O, Nishi K, Osakabe Y. Effect of intraocular lenses on preventing posterior capsule opacification: design versus material. J Cataract Refract Surg. 2004;30(10):2170-2176.
INDICATIONS:
Indicated for primary implantation for the visual correction of aphakia in adult patients in whom the cataractous lens has been removed by an extracapsular cataract extraction method. The lens is intended for placement in the capsular bag.
WARNINGS:
Physicians considering lens implantation under any of the following circumstances should weigh the potential risk/benefit ratio:
1. Recurrent severe anterior or posterior segment inflammation or uveitis.
2. Patients in whom the intraocular lens may affect the ability to observe, diagnose, or treat posterior segment diseases.
3. Surgical difficulties at the time of cataract extraction, which might increase the potential for complications (eg, persistent bleeding, significant iris damage, uncontrolled positive pressure, or significant vitreous prolapse or loss).
4. A distorted eye due to previous trauma or developmental defect in which appropriate support of the IOL is not possible.
5. Circumstances that would result in damage to the endothelium during implantation.
6. Suspected microbial infection.
7. Children under the age of 2 years are not suitable candidates for intraocular lenses.
8. Patients in whom neither the posterior capsule nor zonules are intact enough to provide support.
PRECAUTIONS:
Do not attempt to resterilize the lens as this can produce undesirable side effects. Do not soak or rinse the intraocular lens with any solution other than sterile balanced salt solution or sterile normal saline. Do not store the lens at a temperature greater than 43°C (110°F). DO NOT FREEZE. Do not autoclave the intraocular lens. Do not reuse the lens. It is intended for permanent implantation. If explanted, sterility and proper function cannot be assured. For complete physician labeling information, refer to the enVista™ product package insert.
enVista Toric Specification Sheet
Click Here